
What Is Pseudostrabismus in Babies? A Marietta Parent’s Complete Guide

Pseudostrabismus is a harmless optical illusion in which a baby’s eyes appear crossed or misaligned, even though they are perfectly straight. It is caused by normal infant facial features — most commonly wide nasal bridges and epicanthal folds — and typically resolves on its own by 18 months as the baby’s face matures. No treatment is required, but a professional evaluation is strongly recommended to rule out true strabismus.
You noticed it in a photo — or maybe in person — and your heart skipped a beat. Your baby’s eyes look crossed. Before worry takes over, take a breath. What you may be seeing is one of the most common and harmless optical illusions in infant development: pseudostrabismus.
At Cook Vision Therapy Center, Inc. in Marietta, GA, we work with parents just like you every day — parents who are sharp, attentive, and deeply invested in their child’s health. Our goal with this guide is to give you clear, expert-level answers so you can move from anxiety to understanding, and know exactly when — and whether — to seek professional care.
Understanding Pseudostrabismus — The “Optical Illusion” Explained
Pseudostrabismus is not a disease, a disorder, or a sign that something is wrong with your baby’s eyes. The word itself tells the story: pseudo means false. Your baby’s eyes are, in fact, pointing in exactly the right direction. What creates the illusion of misalignment is the structure of your baby’s face, not the alignment of the eyes themselves.
In the earliest months of life, most babies have a wide, flat nasal bridge and small folds of skin near the inner corners of their eyes. These features partially cover the white part of the eye (the sclera) on the inner side, making the colored part of the eye (the iris) appear shifted — as if one or both eyes are drifting inward. The result is an appearance of crossed eyes that simply does not reflect what the eyes are actually doing.
Pseudostrabismus is extremely common, particularly in babies from birth through approximately 18 months of age, and it is one of the leading reasons parents of infants contact pediatric eye specialists across the Metro Atlanta area.
| Feature | Pseudostrabismus | True Strabismus |
|---|---|---|
| Eye alignment | Correctly aligned | Genuinely misaligned |
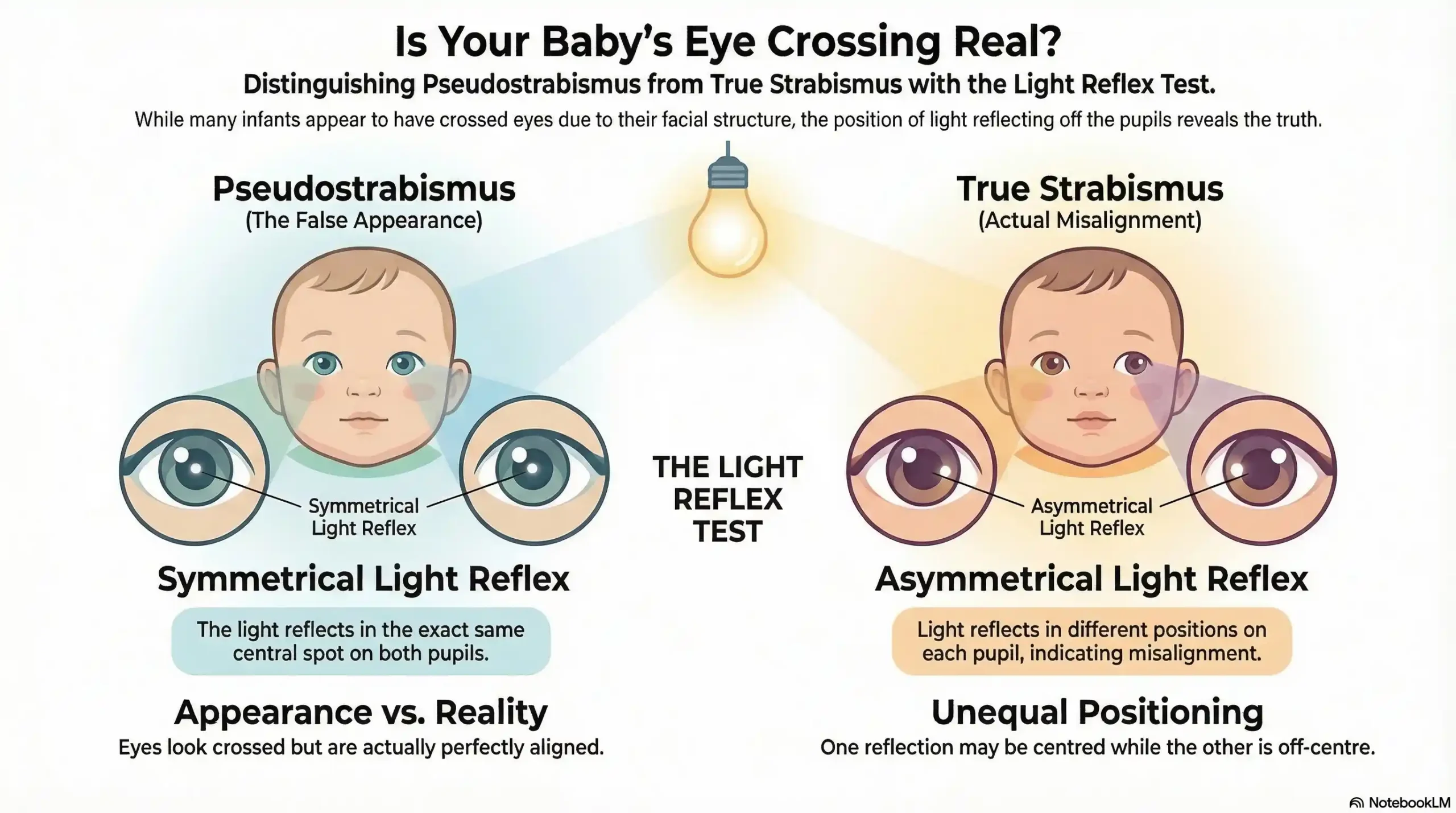
| Light reflex (flash photo) | Reflects equally in both pupils | Reflects at different points |
| Cause | Facial structure (nasal bridge, eyelid folds) | Muscle imbalance, neurological, or refractive |
| Resolves with age? | Yes, typically by 18 months | No — requires professional treatment |
| Vision impact | None | Can lead to amblyopia if untreated |
| Treatment needed? | No | Yes — vision therapy, glasses, or other intervention |
What Causes Pseudostrabismus in Babies?
Understanding the cause of pseudostrabismus helps demystify the appearance and gives parents an accurate framework for monitoring their child’s development.
Epicanthal Folds
Epicanthal folds are small, vertical folds of skin that cover the inner corner of the upper eyelid. They are entirely normal in newborns and young infants and are especially prominent in babies of Asian descent, though they can appear in children of any ethnicity. These folds reduce the visible white space between the iris and the inner eyelid, creating the optical impression that the eye is turning inward — a condition called pseudoesotropia, and the most common form of pseudostrabismus.
Wide or Flat Nasal Bridge
A wide or flat nasal bridge is the most frequently cited cause of pseudostrabismus in infants. Because the nasal bridge is the visual anchor between the two eyes, a wider bridge makes the eyes appear closer together and angled inward — even when they are perfectly parallel and working together in complete harmony.
Eyelid Shape and Coverage
In some babies, the upper eyelid partially covers the colored iris, particularly when the baby looks to one side. This creates an asymmetric appearance that can be mistaken for an eye turn, especially in photographs taken slightly off-center.
Who Is Most at Risk?
While pseudostrabismus can appear in any infant, it is most commonly observed in:
- Babies with a naturally broad or flat nasal bridge
- Infants of East Asian, Southeast Asian, or certain Indigenous heritage, due to more prominent epicanthal folds
- Premature infants, in whom certain retinal and macular features may create related optical effects
- Babies where the appearance is especially noticeable in flash photography, as off-center angles amplify the illusion
Pseudostrabismus vs. True Strabismus — Know the Difference
This is the question that brings most parents to our clinic — and it is exactly the right question to ask. The distinction between pseudostrabismus and true strabismus is not merely academic. It is the difference between a harmless quirk of facial development and a condition that, if left unaddressed, can permanently affect your child’s vision.
📞 Not sure what you’re seeing in your baby’s eyes? Call Cook Vision Therapy Center at (770) 419-0400 for a Free Phone Consultation. Our team will listen, answer your questions, and let you know whether an in-person evaluation makes sense — no pressure, just honest guidance from experts who care.
Key Differences at a Glance
| Category | Pseudostrabismus | True Strabismus |
|---|---|---|
| Appearance | Eyes look crossed in photos or at certain angles | One eye consistently drifts in, out, up, or down |
| Consistency | Often varies with viewing angle | May be constant or intermittent |
| Age of onset | Birth to 18 months | Any age; most common before age 6 |
| Self-resolving | Yes | No — worsens without intervention |
| Risk of amblyopia | None | High if untreated |
| Diagnosis method | Hirschberg light reflex test | Cover test, full vision evaluation |
The At-Home Flash Photo Test
One practical, parent-friendly screening tool is the flash photograph test. Here is how to perform it:
- Position your baby so they are looking directly at the camera.
- Take a flash photo in a normally lit room.
- Examine where the light reflects inside each eye (the corneal light reflex).
In a baby with pseudostrabismus, the flash reflection will appear at the same spot in both pupils — typically in the center. In a baby with true strabismus, the reflection will appear at a different point in each eye, indicating genuine misalignment.
While this test is a useful first observation tool, it is not a substitute for a professional evaluation. A trained clinician can detect subtle or intermittent eye turns that even careful parents and cameras will miss.
Why This Distinction Matters for Your Baby’s Future Vision
True strabismus, left untreated, does not simply improve with time. The brain, receiving two conflicting images, will begin to suppress the input from the misaligned eye. Over time, this suppression leads to amblyopia — commonly known as lazy eye — a condition in which the visual pathways in the brain fail to develop properly. Vision lost to amblyopia in early childhood is significantly more difficult to recover later. Early detection and intervention are the most powerful tools available to protect your child’s long-term visual function.
Does Pseudostrabismus Go Away on Its Own?
In the vast majority of cases, yes — pseudostrabismus resolves naturally as a baby grows. As the first year of life progresses, the nasal bridge becomes more defined and elevated, the epicanthal folds become less prominent, and the face develops proportions that reveal the eyes’ true, straight alignment. By 18 months of age, most cases of pseudostrabismus have significantly improved or disappeared entirely.
However, not every case follows this timeline. In some children — particularly those with certain genetic backgrounds or facial structures — the epicanthal folds may remain more prominent into toddlerhood or even beyond. In these cases, the appearance may persist longer without indicating any problem with the eyes themselves.
The more important question is not whether the appearance has resolved, but whether what you are seeing is truly pseudostrabismus — or whether a real eye turn has been present all along.
Warning Signs: When “Fake” Crossed Eyes May Be Something More
A diagnosis of pseudostrabismus from a qualified clinician is genuinely reassuring. However, it should never lead to complacency. Research indicates that a meaningful percentage of children initially identified with pseudostrabismus are later found to have developed true strabismus. This is why professional monitoring — not just parental observation — is the standard of care.
| Warning Sign | What It May Indicate |
|---|---|
| One eye consistently drifts in a specific direction | Possible true esotropia or exotropia |
| Eye turn is becoming more frequent or more pronounced | Condition may be progressing |
| Child tilts or turns their head to look at objects | Compensating for a true misalignment |
| Child frequently squints or covers one eye | Possible double vision or suppression |
| Family history of strabismus or amblyopia | Elevated genetic risk — earlier evaluation needed |
| Appearance has not improved by 18 months | Professional re-evaluation is essential |
| Flash photo test shows unequal light reflex | Warrants immediate clinical assessment |
⚠️ If you are observing any of these signs in your child, please do not adopt a “wait and see” approach. Contact Cook Vision Therapy Center at (770) 419-0400 today. Early detection makes an extraordinary difference in outcomes. Our practice is located at 1395 South Marietta Pkwy SE, Bldg 400, Ste 107, Marietta, GA 30067, proudly serving families throughout Cobb County, Metro Atlanta, and the greater Southeast.
The 12% Rule — Why Professional Monitoring Matters
Published research and clinical experience suggest that approximately 1 in 8 children initially identified with pseudostrabismus will go on to develop true strabismus. This figure underscores a critical point: a reassuring initial finding does not eliminate the need for ongoing, professional monitoring. The window for the most impactful treatment of strabismus and amblyopia is the early childhood years — a window that cannot be reopened once it closes.
What a Comprehensive Vision Therapy Evaluation Includes
At Cook Vision Therapy Center, our pediatric vision evaluations go far beyond a simple acuity check. A comprehensive assessment examines visual acuity, binocular vision function, eye movement control, focusing ability, and visual processing — providing a complete picture of your child’s visual development at every stage.
How Is Pseudostrabismus Diagnosed? The Professional Evaluation Process
Accurately distinguishing pseudostrabismus from true strabismus requires more than observation. It requires a structured clinical evaluation performed by a qualified vision specialist. Here is what that process involves:
The Hirschberg Corneal Light Reflex Test
The Hirschberg test is the primary tool used to assess eye alignment in infants who cannot yet cooperate with more complex testing. A light is directed at the baby’s eyes, and the clinician observes where the reflection appears on the cornea of each eye. Symmetric reflections indicate proper alignment. Asymmetric reflections indicate a genuine eye turn.
The Cover-Uncover Test
In cooperative patients, the cover-uncover test provides definitive information about eye alignment. Each eye is covered and uncovered in turn while the child fixates on a target. Any movement of the uncovered eye as the other is covered indicates a true strabismus. In pseudostrabismus, no movement occurs — the eyes are already aligned.
Cycloplegic Refraction — Ruling Out Hidden Farsightedness
One critical component of a thorough evaluation is cycloplegic refraction — the use of dilating drops to temporarily relax the eye’s focusing muscles and obtain an accurate measurement of the child’s refractive error. High degrees of farsightedness (hyperopia) can cause the eyes to cross when attempting to focus, producing accommodative esotropia — a true strabismus that can be missed if refractive error is not properly assessed.
Why a Routine Pediatrician Check Is Not Enough
A standard pediatric wellness exam includes a basic vision screening, but these screenings are not designed to detect the subtle binocular vision issues that distinguish pseudostrabismus from early strabismus. They measure visual acuity — how clearly a child sees — not how the eyes work together as a team. Only a comprehensive evaluation by a developmental or behavioral optometrist can provide that level of assessment.
Treatment for Pseudostrabismus — What Parents Need to Know
Pseudostrabismus itself requires no treatment. The condition is a normal feature of infant facial development, and it will resolve naturally in the vast majority of children as their facial proportions mature. Parents should resist any recommendation to pursue surgical or cosmetic intervention for a confirmed case of pseudostrabismus alone.
What is required is vigilance. Because pseudostrabismus and true strabismus can coexist, and because true strabismus can develop after an initial diagnosis of pseudostrabismus, regular monitoring by a qualified clinician is essential.
If a true strabismus is identified during or after the evaluation process, non-surgical vision therapy offers a powerful, personalized pathway to treatment. At Cook Vision Therapy Center, our approach is grounded in four decades of clinical experience and a genuine commitment to non-surgical, lasting solutions. Vision therapy works by retraining the visual system — helping the brain and the eyes learn to work together as a coordinated, efficient team. The result is not just straighter eyes, but improved 3D vision, better eye-body coordination, and a foundation for lifelong visual performance.
🏛️ Local Resources & Citations
1. Georgia Department of Public Health — Health Check Program The official Georgia state program (.gov) that mandates pediatric vision, hearing, dental, and developmental screenings for children — use this resource to understand your child’s state-required screening schedule and locate a certified Health Check provider near Marietta.
2. Cobb/Douglas Public Health District — Georgia DPH The official Cobb County public health office (.gov) serving Marietta and surrounding communities — contact this office to obtain or verify the required Georgia Certificate of Vision Screening (Form 3300) needed for school enrollment in the Cobb County School District.
3. Cobb County School District — Student Enrollment & Vision Screening Requirements The official Cobb County School District portal (.org) detailing the mandatory Georgia Form 3300 Vision, Hearing, Dental, and Nutrition Screening Certificate required for all kindergarten and new-enrollment students — refer here to confirm deadlines and document requirements before your child starts school.
4. Georgia.gov — Required Health Records to Attend School The official State of Georgia portal (.gov) that outlines all health screening certificates legally required for school enrollment — including the vision screening requirement — helping Marietta parents understand exactly which official documents a comprehensive pediatric vision evaluation can fulfill.
Why Marietta Parents Trust Cook Vision Therapy Center
When it comes to your child’s vision, experience, expertise, and genuine compassion are non-negotiable. At Cook Vision Therapy Center, Inc., these qualities are built into everything we do.
Our founder, Dr. David L. Cook, O.D., F.A.A.O., F.C.O.V.D., is an internationally recognized clinician, educator, and author with over 40 years of experience treating pediatric vision conditions — including strabismus, amblyopia, convergence insufficiency, and the full spectrum of vision-related developmental challenges. He is the author of Visual Fitness and When Your Child Struggles, two landmark publications that have guided parents and clinicians alike.
Alongside Dr. Cook, Dr. Ekta Patel, B.Optom, O.D. brings her own deep commitment to personalized, patient-centered care to every evaluation and therapy session.
Our philosophy is simple: we do not offer one-size-fits-all solutions. We tailor the best in vision therapy to meet your child’s unique challenges — because every patient deserves a plan as individual as they are.
We proudly serve families from across Marietta, Kennesaw, Roswell, Duluth, Cobb County, and the broader Metro Atlanta region, as well as patients traveling from across the Southeast — including Chattanooga, Birmingham, and Charleston — and across the nation.
🟢 Begin Your Journey to Restored Visual Performance Today.
If you have concerns about your baby’s eye alignment — whether you suspect pseudostrabismus or true strabismus — we are here to help. Our team offers a Free Phone Consultation to help you understand your child’s visual health and determine the right next step.
📍 Cook Vision Therapy Center, Inc. 1395 South Marietta Pkwy SE, Bldg 400, Ste 107, Marietta, GA 30067 📞 (770) 419-0400 🌐 cookvisiontherapy.com
Your child’s vision is their window to the world. Let’s make sure that window is clear.
Frequently Asked Questions
-
Yes, pseudostrabismus resolves on its own in the vast majority of cases. As a baby’s face matures, the nasal bridge becomes more defined and prominent epicanthal folds become less visible — typically between 6 and 18 months of age, with most cases fully resolved by age 2 to 3. No treatment is required. However, if the crossed-eye appearance has not improved by 18 months, a professional evaluation is strongly recommended to rule out true strabismus.
Disclaimer:
This article is for educational purposes only and does not replace a professional eye examination. If you notice persistent eye misalignment or any concerning changes in your child’s vision, consult a qualified pediatric eye care specialist for an accurate diagnosis.


